ACCC's Improving Care Coordination Model can lead to improved care and treatment outcomes for patients with lung cancer.

Lung cancer is the leading cause of cancer deaths worldwide. It is most often diagnosed at an advanced and incurable stage. Patients suspected of having lung cancer undergo a complex process to diagnose, stage, and treat the disease. Due to the advanced stage of disease at diagnosis, patients often need to undergo multiple tests and evaluations. Care coordination—the coordinated effort to deliver care—has been shown to not only improve the quality of care, but also improve health outcomes for patients.
In 2020, the Association of Cancer Care Centers (ACCC) developed the Improving Care Coordination (ICC) Model which built upon the Multidisciplinary Care (MDC) Assessment Tool created by the National Cancer Institute’s Community Cancer Centers Program (NCCCP). Both models looked to improve the quality of multidisciplinary care which would lead to improved quality of life and treatment outcomes for patients.
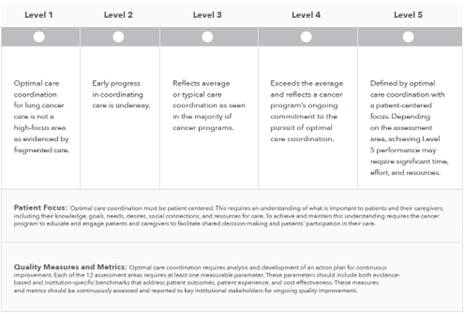
The Model is a framework that includes 12 assessment areas with 5 levels. Within each level are service-asset criteria, with Level 1 representing the most basic provision of care and Level 5 representing the optimal best practice for care coordination. The Model is intended to help cancer programs and practices improve to any achievable target level within a selected assessment area.

The Model is intended to be used by a multidisciplinary team that cares for patients with cancer, including oncologists, hematologists, physician assistants, nurse practitioners, pharmacists, social workers, financial advocates, and administrators. The Model supports an objective assessment on how cancer care is provided at an institutional level. Further, while the Model was originally created to improve care coordination for lung cancer patients covered by Medicaid, it serves as a scaffolding to build quality improvement initiatives focused on care coordination for all patients. The Model can be utilized across all cancer types and oncology centers.
When a cancer program or practice employs the Model to assess its current state of care coordination, it is likely to find its performance includes some components of 1 level and some of another. As a framework, the Model’s purpose is to help cancer programs and practices objectively identify where opportunities exist to improve care coordination for patients, rather than be concerned with reaching a certain level in a specific assessment area.
The 12 assessment areas should be evaluated on their own merits. However, as a cancer program or practice begins to work with the Model, it is likely to find that improvement in optimal care coordination in 1 assessment area often depends on improvements in other areas. And, conversely, improvements in 1 assessment area will often lead to synergistic improvements in other areas. Additionally, although the Model is intended as an internal evaluation tool, cancer programs and practices may benefit from having an unbiased external evaluator complete the self-assessment.
Continuous quality improvement (CQI) in health care is vital to providing quality patient care and maintaining satisfaction among providers and patients. The goal of CQI is to make gradual improvements in operating processes, safety (ie, improved work environment), and patient care. The ICC Model is a tool that can support cancer programs and practices in evaluating strengths and areas that need improvement in the pursuit of optimal patient care. Each of the assessment areas has 5 levels, with level 1 representing the most basic provision of care and level 5 representing the achievement of optimal best practice.
The ICC model aims to help cancer programs and practices improve to any achievable target level within a selected assessment area. Although the Model was originally developed for the lung cancer population, many components of the Model can be used across the cancer care delivery system, independent of patient tumor type.
Has your program used the Model? Let us know! Send your thoughts to Lilly Meier.
Recent work to update the ICC Model is made possible by support from Regeneron.